Updates in human and health sectors in Iraqi Kurdistan: a war-torn region
Faiq B.Basa,1 Sivar A. Qadir,2 Haveen H. Alsilefanee,3 Luma H. H. Alhanabadi,4 Shahla O. Salih,5 Gorgees S. Akhshirsh,6 Bayar S. Azeez,6 Moramarco S.7
1 Rizgary Teaching Hospital, Erbil, Kurdistan Region, Iraq
2 Directorate of Health, Sulaimaniya, Kurdistan Region, Iraq
3 Family Medicine, Directorate of Health, Duhok, Kurdistan Region, Iraq
4 Primary Health Care Department, Preventive Health Affairs Directorate, Duhok, Kurdistan Region, Iraq
5 Department of Statistics and Informatics, University of Sulaimaniya, Iraq
6 Computer Systems Engineering, Erbil, Kurdistan Region, Iraq
7 University of Rome Tor Vergata, Italy
Setting
Throughout decades, Iraq has endured several conflicts and socio-political tensions, at both national and international level, that have deeply impacted the country asset, engendering a country still politically unstable and socially fragile, as highlighted by several development indexes:
- The Sustainable Development Goals (SDG) Index score is an index scoring a country’s position between the worst (0) and the best or target (100) outcomes. When considering sustainable development, Iraq is ranking at the 127th position out of 156. In 2018, the total SDG score index for Iraq was 53.7, with most critical areas identified as food security and sustainable agriculture (SDG2), inclusive and equitable quality education (SDG4), building resilient infrastructure and sustainable industrialization (SDG9), reducing inequalities within and among countries (SDG10) - for which no data are available - conserve and sustain use of marine resources (SDG14).2
- The UNDP’s Human Development Index (HDI), launched in 1990, captures human progress, combining information on people’s health, and education. Over the years, the HDI has served as a comparative tool of excellence, and as a platform for national priorities; index’s dimensions include life expectancy, education and standard of living. The index can ideally range from 0 (very low) to 1 (very high). Iraq’s HDI for 2017 was 0.685 (medium value), posing the country at the 120th position out of 189 countries.1
- The Gender Inequality Index (GII) measures disparities on the HDI by gender, capturing the inequalities women face in reproductive health, education, political representation and the labor market. The higher the GII value, the greater the gender inequality, with 0 being 0% inequality and 1 being 100% inequality. In 2017 Iraq’s GII scored 0.506, posing the country at the 123th position.1 This shows a country at medium human development, where gender inequality still exists.
- The Multidimensional Poverty Index (MPI) calculates the number of persons experiencing poverty in multiple and simultaneous ways and the average number of deprivations.3 The global MPI is an index of acute multidimensional poverty that covers over 100 countries. It was developed in 2010 to replace the Human Poverty Index. It can range from 0 to 1 (weighted average of 10 indicators categorized in three dimensions of deprivations: health, education and standard of living), where a higher number signifies greater poverty. The 2018 report - which for Iraq presents data updated at 2011 from the Multiple Indicator Cluster Survey (MICS) - shows for Iraq a quite low MPI (0.059), with 14.7% of the population that is multi-dimensionally poor,4,5 with the 2.5% of people living below the $1.90 a day poverty line.6
- The Fragile States Index (FSI) is a ranking of 178 countries across the sum of 12 different indicators (cohesion, economic, political, legal, social).7 Тhe FSI assesses the risks and vulnerabilities faced by individual nations – the lowest (0) for sustainability and the highest (120) for alert. The FSI scores should be interpreted with the understanding that the lower the score, the better. The index, based on The Fund for Peace’s proprietary Conflict Assessment System Tool (CAST) analytical approach, is determinant to understand more about a state’s capacities and pressures which contribute to levels of fragility and resilience. Despite final victory was declared against the so called Islamic State-ISIS and a relative stability returned to some recently conflicted parts of the country, nowadays Iraq continue to experience high levels of instability. Its FSI in 2018 was 102.2, posing the country at high state of alert.
However, the Kurdistan Region of Iraq (KRI), in the north of the country, has experienced different conditions from the rest of Iraq, enjoying a better security environment in the last years. After a series of conflicts with different political regimes, the KRI progressively slipped out of Baghdad’s control and became autonomous from the central government in 1991, under United Nations auspices. In 2005, the Iraq’s Constitution recognized the Kurdistan Regional Government (KRG). The comparison between the internally displaced people (IDPs) in the KRI and other Iraqi regions witness this finding: during the 2014–2017 crisis, the KRI has been perceived as a “safe haven” by Iraqis fleeing, as well as by Syrian refugees.8
Over the years, the KRI continued to desire for independence from Baghdad, culminated launching a referendum in September 2017. Despite the result was overwhelmingly in favor of independence, the central Iraqi government rejected the vote as unconstitutional. Nowadays, the Autonomous Region of Kurdistan (RAK) - administratively divided into four governorates: Duhok, Erbil, Sulaymaniya, Halabja - hosts a molting pot of population consisting of Kurds, Assyrians, Chaldeans, Turkmen, Armenians and Arabs.
Demographic Overview
The last census in Iraq was conducted in 1997. However, the census excluded the population of some KRI governorates, due to the impact of the Second Gulf War on these governorates. Another census was scheduled for 2007, but due to the exceptional circumstances that followed the fall of the regime, it was never completed. Only a quick count of the population, carried on with the process of numbering and listing the housing, was conducted at the end of 2009.9 At July 2018, the last Iraqi demographic survey estimated a general population counted up to 40,194,216 people.10 Тhe last available age structure of Iraq shows a larger proportion of population in the younger age groups, with 39% under 15 years of age. The median age of the population is 20.2 years. Life expectancy at birth in 2016 was reported to be 68/72 years.
As specific regard of the Kurdistan Region, for more than 30 years (since last census in 1997) the socio-demographic and living conditions of the Kurdish population have not been statistically monitored and only estimations have been provided.8 Traditionally, the majority of people lived in villages and survived on farming, but when Saddam Hussein’s regime destroyed over 4,000 villages, in the 1980s, people were forced to move to towns and cities.11
Nowadays, national estimated data report a population of nearly 5,2 million people,11 with the 68.8% of the population living in urban area. The 35% of the population is younger than 15 years, 61% belongs to the active age groups and 4% is 65 or above. The median age of the population is 19.5 years.12 In 2017 the population pyramid showed to be of the expansive type, with a wide base and a triangular shape, typical of a developing nation with a large share of young population.11
Internally displaced people (IDPs), refugees and people of concern
KRI demography changed considerably because of wars and conflicts: during the regime, tens of thousands people were killed, while the last recent decades of political instabilities and armed conflict in Iraq and neighboring countries have deeply impacted the human tool of displacement, seeking for a safest place in KRI. More recently, the rise of the so called Islamic State of Iraq and Syria (ISIS) led to the 2014–2017 crisis, starting with an additional 1 million people forced to flee their homes (in 2014, over 2.5 million civilians were already displaced in Iraq and a similar number had emigrated abroad). At the beginning of 2015, the total number of refugees and IDPs added up to 1.5 million in KRI (the only pretty safe area in the country), which constitutes nearly a 30% increase in KRI’s population. This human load have completely changed the demographic asset of the region over the years, and has put even more pressure on the already debilitated health system and local services.13 With the military operation to retake Mosul, between October 2016 and July 2017, more than 3 million people were displaced. In December 2017, the Government of Iraq announced the cessation of hostilities after the retaking of areas previously held by the so called Islamic State-ISIS. Since then, the number of IDPs has declined as people gradually returned to their homes and communities. At the end of October 2018, the data of the International Organization of Migration (IOM) Displacement Tracking Matrix (DTM) (Round 106) collection across 18 governorates, identified 1,866,594 IDPs (311,099 families) displaced across 104 districts, 18 governorates and 3,363 locations in Iraq. For the same period, 4,113,624 people returned (685,604 families) across 8 governorates, 29 districts and 1,568 locations, – retaken areas previously occupied by ISIS.14
Actually, the KRI is still hosting the largest numbers of protracted IDPs (as for the end of 2018 more than 30%, disaggregated into 18% of the total number for Duhok Governorate, 11% for Erbil Governorate, and 8% for Sulaymaniyah Governorate)15 and refugees (99% of the 253,672 Syrian refugees currently live in KRI).16 The most updated data of the Ministry of Interior of Iraqi Kurdistan Region reports 1,127,400 total IDPs and 249,639 total refugees for November 2018. Although major efforts are being made by the Government of Iraq and Kurdistan Regional Government to incentivize and facilitate returns, many vulnerable families were still unable to return without assistance, facing widespread unemployment and deterioration of public services.17 As of April 2019, the UN Refugee Agency identified in the country a total of 6,302,786 people of concern, 1,744,980 of which were IDPs as of February 2019.18 Data of the 2018 Iraq Humanitarian Response Plan (HRP), developed to target populations in critical need, reveal that there are millions of people in post-conflict realities still needing protection and support. Agricultural production has declined to 40% compared to pre-conflict levels, with a poverty rate in the most impacted areas exceeds 40%. Nearly 1.9 million are food insecure; more than 7 million people require health care and more than 5.2 million protection support; more that 5.4 million people need water and sanitation assistance and 4.1 million people need shelter. The health sectors have been particularly hard-hit: as examples, in the Governorate of Salah al-Din, nearly one third of health centers are currently damaged or destroyed, while in Ninewa only half of health facilities are fully functional. Conversely, the number of health consultations has increased eightfold since 2014. More than 140,000 vulnerable residents in host communities in the KRI are also estimated to require humanitarian assistance.19 Approximately 130 thousand individuals (the 3% of the total returnee population) were categorized as living in critical shelters.20 Pressures on local services (including schools, water and sanitation, solid waste management, health facilities) and competition for jobs have increased each year, contributing to a sharp decline in living standards across the three governorates.21 In total, 11 camps were closed and consolidated: 4 in Erbil Province, 6 in Duhok province and 1 in Sulaymaniyah province. Currently, total camps in KRI are 38.22 This data are quite in contrast with those of DMT ROUND 106, since report Erbil at the first place for number of IDPs and refugees (49% - total number 678,145), followed by Duhok and Sulaymaniyah (respectively 34% - total number 473,486 and 16% - total number 225,408). More than 706,000 people living in the KRI required some form of humanitarian assistance in 2018. More than 270,000 people needed some form of humanitarian assistance in Dohuk Governorate, more than 350,000 in Erbil, more than 100,000 in Sulaymaniyah.23
The Health System
An historical overview of Iraq’s situation
The Iraqi healthcare sector was experiencing a period of rapid modernization in the 1950s, when the Iraqi Ministry of Health was founded, fueled by rising oil production and prices.24 In the 1970s and 80s, the Iraqi health system used to be one of the best and most advanced in the Eastern Mediterranean Region (EMR), reporting the best health indicators among the overall region. The country boasted free health care in 172 hospitals and 1200 primary health-care clinics.25 Iraqi medical graduates often received specialty training and certification in the UK and Germany.26
The capacity and performance started to deteriorate during the 1980s, then exacerbating in the last decades as a result of continuous wars, sanctions, loss of health workers, looting, and political interference, political and economic sanctions. The health sector was one of the most hard-hit indeed. Health structures collapsed, while many health professionals were killed or forced to flee, causing a shortage of personnel. Huge was the loss of human resources and talents, and further diverted resources and medical staff from civilian facilities, even because many medical doctor, health professionals and young graduates leaved the country looking for better life conditions and a more comfortable work environment.27
A research published in 2009 measured the changes in numbers of medical specialists at 12 Iraqi tertiary hospitals (in Baghdad, Basra, Erbil and Mosul) between 2004 and 2007. Data available of specialists leaving hospital posts, 39% went elsewhere in Iraq and 61% left the country.28 Most updated health-care data, when available, confirm that the Iraqi population is paying a crippling price for the continuing violence, political infighting, and widely acknowledged rampant corruption within the health system.29
Nowadays, in spite of much rebuilding, health infrastructure is still not fully restored.30 The 36% of health centers in Salah al-Din were damaged or destroyed and only half of health facilities in Ninewa were fully functional.31 While 7.6 million people were in need of health services in 2018, some 5.5 million individuals are expected to be in need of primary and secondary healthcare services during 2019, a caseload reduction due to continued IDP returns.32 Contrary to the national needs, many skilled health workers and young graduates continue to leave. Therefore, national development plans call for a realignment of the health system with primary health care as the basis.33
An historical overview of the KRI’s situation
The long-term consequence of years of political instabilities have caused enormous health challenges.34 Before 90s, the Kurdish health infrastructures were in state of abandonment because of policy pursued by the regime of Saddam Hussein: the regime’s persecution made impossible to invest in buildings, equipment and manpower, necessary to sustain modern medical practice and support the needs of a growing population. After his fall, the leaders of Kurdistan Region needed to rebuild the area’s economic and social infrastructure.35
From 1992 to 2003, health balance was just sufficient to cover the salaries of the few health workers. Funding to build or restructure hospitals and other health facilities was not provided. From 2003, the quote for health, guaranteed from the Government of Baghdad to the Kurdistan Region, covered not more than the 40% of the health need.
The Iraqi MoH report in 2004 stated that “the regime which ruled Iraq during the last three decades did not consider health a priority; the health system, therefore, suffered from progressive neglect and budgetary allocations did not reflect population needs. As a result, health indicators fell to levels comparable to some of the least developed countries”.36
Health expenditures followed a positive trend between 2008–2011, when KRG moved to develop the region and improve its citizens’ well-being. In fact, in 2008-2009, 35 new primary health care facilities and 9 new hospitals were built. In this same period, 380 new hospital beds and 25 new operation rooms were added to existing hospitals.37
Between October 2012 and September 2014, because of increased population due to IDPs and refugees, the host communities in KRG were deprived of health spending, with implications for overall health system performance. In 2014, the Ministry of Health of the Kurdistan region of Iraq was reporting critical shortages in medicines and was requesting support from the World Health Organization (WHO) in the provision of urgently needed supplies.38 Since the Syrian crises led KRG to a major increase in demand in the health sector, in 2015 the World Bank conducted an Economic and Social Impact Assessment (ESIA) revealing concern for the negatively impact of the future burden of disease and other health outcomes in the absence of a budget increase. In light of this, higher utilization levels of both primary health care and hospital services were expected, with significant financial additional resources (additional $317 million) required to restore stability to the health sector.39
The health system organization in KRI
Since the creation of the KRG, health service delivery and health financing have been and continue to be a mix of public-private participation and investment. With its establishment in early 1990s, the Ministry of Health (MoH) of Iraqi Kurdistan Regional Government followed the basic organizational structure and system of the Iraqi MoH: public sector services are administered by the Ministry of Health in Erbil, which owns and operates a large network of primary and secondary health care facilities.40 These facilities are financed through general revenues and follow traditional line-item budgeting processes. The Ministry of Finance approves an annual allocation for Ministry of Health services, and all employees are salaried staff under civil service guidelines.39 The KRG decides health policies, which are implemented by MoH, whereas long-term health planning is under the responsibility of the Ministry of Planning (MoP).
The Kurdish health system has many strengths, but also some limits. As in the rest of Iraq, public health system in the Kurdistan Region is organized on two essential levels: nearly sixty public hospitals and hundreds of Primary Health Care Centers (PHCCs). Primary Health Care Centers (PHCCs) are of two types: the main PHCCs, that are located in urban and semi-urban areas, and the smaller PHCCs, that are located in rural areas. Main centers provide a wide range of primary health and dental services, including vaccinations, child growth monitoring, oral rehydration treatment for diarrheal disease, treatment of minor health problems, and health education; some also provide antenatal care and screening and/or management of chronic diseases, such as hypertension and diabetes. Smaller PHCCs provide a more-limited range of services. Very often PHCCs are lacking of adequate equipment, such as laboratory and other diagnostic equipment, as well as information technologies. Nearly all main PHCs have a computer, and nearly all computers are functional. However, a significant number of centers that have a functional computer do not have a trained user, presumably rendering the equipment less than fully useful. This gap is especially true in Erbil.41
Health care is also provided in the private sector in private physician clinics and in private and semiprivate hospitals. The private health sector is strong powerful and has the capacity to supplement the weakness of the public sector especially in curative services. A high number of private clinics are distributed nationwide. The principal funding of the above private facilities is purely private. Almost all medical specialists of private hospitals staff public health care too. Doctors at public sector are allowed by law to practice their profession in the private sector beyond the working hours,42 so that presently most physicians work only a few hours in the public sector before moving to their private-sector clinics.
Health system performance in KRI
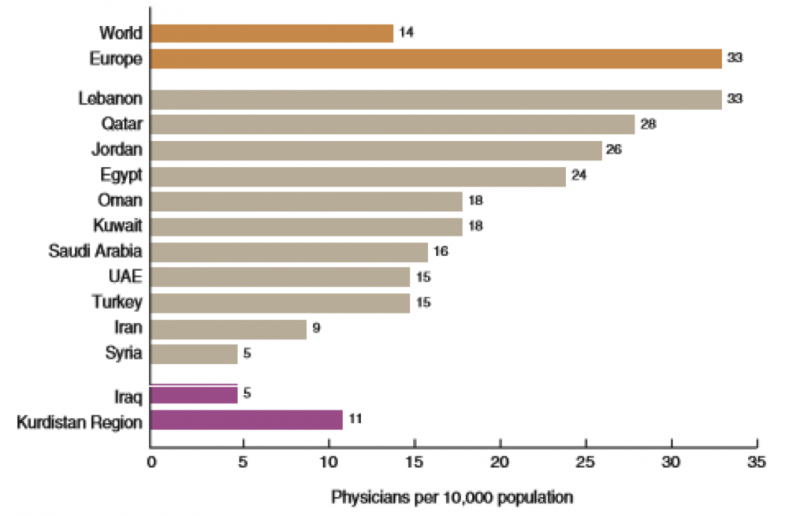
There is a limited documented knowledge about the challenges of the primary care system in the Kurdistan Region (as well as in overall Iraq). Particularly, because health information systems are not systematically used and data collection is not standardized. Figure 1 shows available data (updates of 2008) of the number of physicians per 10,000 habitants in the Kurdistan Region, compared to other Middle-East countries and European and World mean. The KRI has about 11 physicians per 10,000 people. That ratio is lower than in neighboring Arab states, such as Turkey, Lebanon, and Jordan, but higher than in Iraq overall and higher than in impoverished Arab states, such as Syria or countries in northern Africa.41
Figure 1. Physician per 10,000 Population in the Kurdistan Region. (Source: KRG Ministry of Health and WHO 2008)
Since 2010, the RAND Corporation has worked with the MoH and MoP of the KRG to develop and implement initiatives for improving the region’s health and health care system through analysis, planning, and development of analytical tools. One of the most important and feasible recommendations made by RAND was to establish a Management Information System (MIS) to monitor resources and services at PHCCs. Such a system might help monitoring the location, staff, equipment, and services at PHCs across the region and identify problems that require management attention.41
In 2012, the KRI had approximately 6,000 physicians, with approximately 1,400 of them (about 25%) being general doctors/practitioners. RAND research conducted before the refugee crisis found that if the population continued to grow at current rates and KRI physician utilization rates were similar to nearby countries, the KRI would need an additional 2,097 physicians by 2020 (an increase of more than 33%). If the previous estimate was correct, then the KRI needed approximately 1,000 more physicians than it had in 2015 even before counting the need to service IDPs and refugees.43
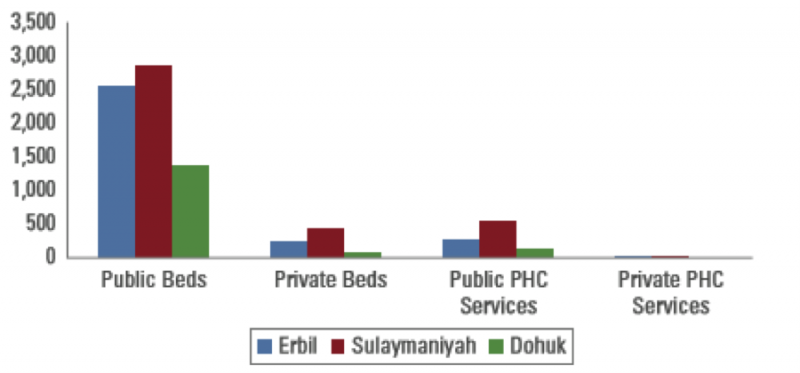
Based on World Health Organization (WHO) recommended standards of two or three centers per 10,000 population, most of the KRG’s main PHCCs serve too many people (more than 10,000), and most sub-centers serve too few (fewer than 2,000).41 Main centers are typically staffed with at least one general practice physician, plus dentists, pharmacists, nurses, medical assistants, laboratory technicians and administrative personnel staff; sub-centers do not have usually a physician but only nurses and medical assistants staff. Doctors working in main PHCCs are general doctors/practitioners. Generally, in all the Iraq general doctors/practitioners do not receive any formal training after graduation, but a clinical internship of two years and one year working in a remote PHCCs or hospital. Figure 2 shows number of Hospital beds by Governorate (updates of 2011). Bearing in mind that number of bed does not reflect the effectiveness of the hospital and it is not a performance indicator, it is also impressive that the PHCCs services, either public or private, are almost non-existent.
Figure 2. Number of Hospital Beds in Public, Private and Mix sector. Source Kurdistan Regional Statistics Office (KRSO) 2011
Health information of KRI
Until now, in Kurdistan there is no systematic collection of health data. It follows that data systems are often inefficient, poor, data are not readily available and the available ones are not routinely used. In Kurdistan, as well as in Iraq, there is no formal and institutionalized structure with the task of monitoring diseases and analyzing health care needs.42 Overall, few health-related and epidemiologic data are collected.44 Medical records are non-existent for outpatients and they are poor and inadequately maintained in hospitals and in-patient departments.42 Wherever possible, data can be deduced from surveys, census, sample registration, vital registration, household recall for death or United Nations estimates.45
For example, the last available official report with health data made by the Kurdistan Minister of Health through the Management Information System-MIS (year 2009), contains few and fragmented data, merely estimated because have been calculated on the base of samples and do not represent the entire population. As an example, estimated rates of neonatal and infant mortality are significantly lower than data of the rest of Iraq (KRG vs Iraq: 9/1000 vs 25/1000 for the neonatal mortality; 27/1000 vs 36/1000 for the infant mortality). Moreover, there is a strong variation, not explained, in data among Kurdish governorates (Erbil, Duhok and Sulaymaniyah), which seem to be due much more to different methods and/or precision in collecting data than to real differences.
Same incongruences are occurring when referring to under-five mortality rates. First of all, it is not clear what the numbers refer to, probably mortality rates x 100,000. When reporting the main causes of death before 5 years and after, there are no specifications between male and female, neither groups of age over 5 years are separated. Moreover, dubious causes of death, such as hypertension (that is a risk factor) and dyspnea (that is a symptom), have been reported. It is clear that these incongruities could have been due to data only estimates because, given the lack of data collection system, these indicators have been calculated on the base of samples and not on the entire population.
Other most available recent data on child mortality comes from the Multiple Indicator Cluster Survey (MICS)46 done in Iraq in 2011. The MICS was realized on a sample of 36580 and published in 2011, by the Central Statistics Coordination of the Kurdistan Region in collaboration with the Ministry of Health, UNICEF and Iraq Trust Fund. Despites estimated rates are quite concordant when comparing with National data, they are very discordant with the previous estimated reported by the Kurdistan MoH in 2009. The most discordant data in on neonatal mortality in KRG: 9/1000 in 2009 compared to 21/1000 in 2011, while surprisingly an improvement in under-five mortality rate was registered: 41/1000 in 2009 vs 32/1000 in 2011.
Lately, in 2018 the Kurdistan Region Statistics Office (KRSO), UNFPA, and IOM launched the demographic survey of the Kurdistan Region of Iraq (KRI), one of the largest statistical exercises conducted in the region since 1987. The survey provides a comprehensive profile of the current population demographics, gathering information from 13,600 households, including displaced families, in the three KRI governorates of Duhok, Erbil and Sulaymaniyah.8 The overall Infant Mortality Rate (IMR) reported for 2017 was 23/1,000 births, slightly still quite underestimated compared to the overall Iraq available data (25/1,000 in 2017 according to the World bank).
As regards communicable diseases, in the report of 2009, the Ministry of Health gives some data on some communicable diseases and the hospitalization rates of five chronic conditions. Morbidity data are partially pointed out, but because of their sporadic nature and limited reliability they can’t be used neither for epidemiological surveillance nor to address policies and health interventions.
The increased number of displaced people and refugees, with consequently caseload of non-communicable diseases (NCDs) among them, have posed new challenges for local government and humanitarian agencies in the provision of health care, diagnostics and medications. In particular, concern has been risen for the access to care among minority groups displaced by ISIS, such as Yazidis, and other and currently residing in camps in the Kurdistan Region of Iraq.47 Therefore, a major priority of Kurdistan is to develop a well-functioning health information system, essential to respond to the needs of the population, with efforts to be done to improve data accuracy and completeness.33
The Way Forward
One of the main priorities on overall Iraq’s agenda appears to be the reconstruction of a full-fledged public health system.
The Government of Iraq, the Ministry of Planning in Baghdad and the Ministry of Planning in Kurdistan region with support from multiple development partners, are engaged in developing new strategies and plans to meet the challenges of transitioning from a crisis context to sustainable development.
The Government of Iraq has prepared the National Development Plan (NDP 2018-2022) with the support of the United Nations Development Program (UNDP) and other UN Agencies to review and discuss the alignment of plans and policies with the Sustainable Development Goals (SDGs) and identify priorities; it also developed a Poverty Reduction Strategy (PRS) with the purpose of targeting the most vulnerable groups, especially in most deprived and peripheral areas, as well as a Reconstruction and Development Framework (2018-2027).48 Continuation of uninterrupted Primary Health Care services to IDPs in camps remains the priority need, along with maintenance and, where required, enhancement of basic minimum standards of quality of healthcare services. Prevention, control and rapid response to communicable and vaccine-preventable disease outbreaks in previously conflict-affected areas is still a critical health need.
The Ministry of Planning of the KRG has developed a Regional Strategic Development Vision for 2020, with the aim to offer improved health service delivery, with sufficient number of primary health centers, but most especially with defined and specific services to be offered. Health facilities, services, and professionals should be distributed appropriately and fully staffed and resourced to enhance access, coverage, efficiency, and quality of care for the entire population. This required also to develop data and information systems with the aim to collect, analyze and interpret health determinants, health system performances and health status of the population. This system of monitoring and epidemiological surveillance is essential to support evidence-based decision-making, as well as to address humanitarian help;33,49 it will be helpful to support modern health policy development, decision making and the long-term planning.50 Strengthening the epidemiological surveillance is crucial during this phase of reconstruction, allowing the country to move beyond decades of steady systemic stagnation.
To respond to this health priority, the University of Rome Tor Vergata (Italy) and the Ministry of Health of KRI started in 2015 a cooperation to implement an electronic system for epidemiological monitoring and health surveillance in the region. The program has been designed to gather on a day-to-day basis health-related data from the population in an online platform (DHIS 2), using the ICD-10 coding system. By September 2019, 59 health facilities in KRI - Dohuk, Erbil, Halabja, Sulaymaniyah - have been engaged (either hospitals and health centers). The aim is to network the approximately 120 main health centers and hospitals of the region in the next three years.51,52 A subsequent expansion of the health monitoring system to whole Iraq is foreseen in the following years, depending on the country stability.
After decades of conflict, such a functioning system will be essential in guiding the development of appropriate public health interventions since, alongside the necessary early-response intervention, it is the only way to manage in the medium and long term the complex and open-ended social situations that affect population health.53
References
- UNDP. Human Development Indices and Indicators 2018 Statistical Update. 2018.http://hdr.undp.org/sites/default/files/2018_human_development_statistical_update.pdf
- Bertelsmann Stiftung and Sustainable Development Solutions Network. SDG Index and Dashboards Report 2018. Implementing The Goals Global Responsibilities. 2018. http://sdgindex.org/assets/files/2018/01%20SDGS%20GLOBAL%20EDITION%20WEB%20V9%20180718.pdf
- Alkire S, and Jahan S. The New Global MPI 2018: Aligning with the Sustainable Development Goals’, HDRO Occasional Paper, United Nations Development Programm 2018. http://hdr.undp.org/sites/default/files/2018_mpi_jahan_alkire.pdf (2018)
- Oxford Poverty and Human Development Initiative. Global Multidimensional Poverty Index 2018: The Most Detailed Picture to Date of the World’s Poorest People, University of Oxford, UK, 2018. https://ophi.org.uk/wp-content/uploads/G-MPI_2018_2ed_web.pdf
- Global MPI Country Briefing 2018: Iraq (Arab States). Oxford Poverty and Human Development Initiative (OPHI). Country Briefing, December 2018. https://ophi.org.uk/wp-content/uploads/CB_IRQ-3.pdf
- OPHI website. Global comparisons. https://ophi.org.uk/multidimensional-poverty-index/databank/global-comparisons/
- Fund for Peace. Fragile State Index 2018. The Fund for Peace. http://fundforpeace.org/fsi/2018/04/19/fragile-states-index-2018-issues-of-fragility-touch-the-worlds-richest-and-most-developed-countries-in-2018/
- IOM, UNFPA, KRSO. Demographic Survey Kurdistan Region of Iraq. 2018. file:///C:/Users/E411a/Downloads/KRSO_IOM_UNFPA_Demographic_Survey_Kurdistan_Region_of_Iraq.pdf
- Iraq National Population Commission & United Nations Population Fund. Iraq Population Situation Analysis Report 2012
- CIA. The World Factbook Website. https://www.cia.gov/library/publications/the-world-factbook/geos/iz.html#field-anchor-people-and-society-age-structure
- Kurdistan Regional Government Website. The People of the Kurdistan Region. http://cabinet.gov.krd/p/p.aspx?l=12&s=020000&r=304&p=214
- World Meter Website. http://www.worldometers.info/world-population/iraq-population/
- Mowafi H. Conflict, Displacement and Health in the Middle East, Global Public Health, 2011; 6:5, 472-487, DOI: 10.1080/17441692.2011.570358
- IOM Displacement Tracking Matrix (DTM) Round 106- IOM Iraq October 2018. Available at: http://iraqdtm.iom.int/LastDTMRound/DTM%20106%20Report%20English.pdf
- IOM-RWG Iraq Reasons to Remain: Categorizing Protracted Displacement in Iraq. November 2018. Available at: file:///C:/Users/E411a/Downloads/IOM%20RWG%20SI%20Categorizing%20Protracted%20Displacement%20in%20Iraq_November%202018.pdf
- UNHCR. The UN Refugee Agency. Iraq Fact Sheet, April 2019. https://data2.unhcr.org/en/documents/download/69249
- The 2018 Iraq Humanitarian Response Plan (HRP). https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/english_2018_hrp_executivesummary_irq_final_website_0.pdf
- IOM Iraq Displacement Tracking Matrix (DTM) Round 108- IOM Iraq February 2019. Available at: http://iraqdtm.iom.int/Downloads/DTM%202019/February%202019/Round108_Report_English_2019_February_IOM_DTM.pdf
- The 2018 Iraq Humanitarian Response Plan (HRP). Available at: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/english_2018_hrp_executivesummary_irq_final_website_0.pdf
- IOM Displacement Tracking Matrix (DTM) Round 106- IOM Iraq October 2018. Available at: http://iraqdtm.iom.int/LastDTMRound/DTM%20106%20Report%20English.pdf
- The 2018 Iraq Humanitarian Response Plan (HRP). Available at: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/english_2018_hrp_executivesummary_irq_final_website_0.pdf
- Ministry of Interior Joint Crisis Coordination Centre. Registered IDPs and Refugees in Kurdistan Region – Iraq for November 2018. Available at http://jcc.gov.krd/contents/files/18-12-2018/1545127211.Total%20No.%20IDPs%20%20Refugees%20for%20November%20in%20Kurdistan%20Region-Iraq.pdf
- IOM Displacement Tracking Matrix (DTM) Round 106- IOM Iraq October 2018. Available at: http://iraqdtm.iom.int/LastDTMRound/DTM%20106%20Report%20English.pdf
- Al-Bayan Center for Planning and Studies. Restoring the Iraqi Healthcare Sector: The British National Health Service as a Model. 2018
- Middle East Health. Iraq Report. On the Road to Recovery. 2012. http://www.middleeasthealthmag.com/cgi-bin/index. cgi?http://www.middleeasthealthmag.com/jan2012/feature1.htm
- Al Hilfi TK, Lafta R, Burnham G. Health Services in Iraq. Lancet. 2013 Mar 16;381(9870):939-48
- Mokdad Ali H. et al. Health in Times of Uncertainty in the Eastern Mediterranean Region, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet Glob Health. 2016 Oct;4(10):e704-13. Epub 2016 Aug 25
- Burnham GM, Lafta R, Doocy S. Doctors Leaving 12 Tertiary Hospitals in Iraq, 2004–2007. Social Science & Medicine 69 (2009) 172–177
- Webster PC. lraq’s Health System Yet to Heal from Ravages of War: Special Report. The Lancet, Volume 378, Issue 9794, 863 - 866
- Devi S. Reconstructing Iraq. The Lancet, 2018; 392 (10147), 541 - 542 Media Reports Monitored by the International NGO Safety Organization
- The 2018 Iraq Humanitarian Response Plan (HRP). Available at: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/english_2018_hrp_executivesummary_irq_final_website_0.pdf
- UN Office for the Coordination of Humanitarian Affairs. Iraq: Humanitarian Needs Overview 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/irq_2019_hno.pdf
- Al Hilfi TK, Lafta R, Burnham G. Health Services in Iraq. Lancet. 2013 Mar 16; 381(9870):939-48
- Shabila NP, Al-Tawil NG, Al-Hadithi TS, Sondorp E, Vaughan K. Iraqi Primary Care System in Kurdistan Region: Providers’ Perspectives on Problems and Opportunities for Improvement. BMC Int Health Hum Rights. 2012 Sep 27; 12:21.
- RAND Corporation. Strengthening Health Care in the Kurdistan Region of Iraq. Research Brief.
- Alwan A. Health in Iraq. The Current Situation, Our Vision for the Future and Areas of Work. Ministry of Health 2004
- World Bank.2015. The Kurdistan Region of Iraq: Assessing the Economic and Social Impact of the Syrian Conflict and ISIS. Washington, DC:World Bank.doi:10.1596/978-1-4648-0548-6.
- WHO Website. Ministry of Health of the Kurdistan Region of Iraq Reports Critical Shortages in Medicines, Seeks Support from the World Health Organization. Iraq news 2014. http://www.emro.who.int/iraq-press-releases/2014/critical-medicine-shortages.html
- World Bank. The Kurdistan Region of Iraq: Assessing the Economic and Social Impact of the Syrian Conflict and ISIS. Washington, DC:World Bank 2015..doi:10.1596/978-1-4648-0548-6.
- Shabila NP, Al-Tawil NG, Tahir R, Shwani FH, Saleh AM, Al-Hadithi TS. Iraqi Health System in Kurdistan Region: Medical Professionals’ Perspectives on Challenges and Priorities for Improvement. Conflict and Health 2010, 4:19
- Anthony C.R, Moore M, Hilborne L.H., Rooney A. Health Sector Reform in the Kurdistan Region - Iraq Primary Care Management Information System, Physician Dual Practice Finance Reform, and Quality of Care Training. Kurdistan Regional Government Ministry of Planning, Ministry of Health. RAND Corporation 2017
- WHO. Health Systems Profile - Iraq. Regional Health Systems Observatory. 2006. http://apps.who.int/medicinedocs/documents/s17295e/s17295e.pdf
- Moore, Melinda, C. Ross Anthony, Yee-Wei Lim, Spencer S. Jones, Adrian Overton, and Joanne K. Yoong, 2014. The Future of Health Care in the Kurdistan Region - Iraq: Toward an Effective, High-Quality System with an Emphasis on Primary Care, Santa Monica, Calif.: RAND Corporation and Ministry of Planning of the Kurdistan Regional Government, MG-1148-1-KRG, 2014.
- Webster PC. Iraq’s Health System Yet to Heal from Ravages of War. Lancet. 2011 Sep 3;378(9794):863-6
- Health in Times of Uncertainty in the Eastern Mediterranean Region, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013
- The Central Statistics Organization and the Kurdistan Regional Statistics Office. 2012. Iraq Multiple Indicator Cluster Survey 2011. Final Report. Baghdad, Iraq: The Central Statistics Organization and the Kurdistan Regional Statistics Office
- Cetorelli V, Burnham G, Shabila N. 2017. Prevalence of Non-Communicable Diseases and Access to Health Care and Medications among Yazidis and Other Minority Groups Displaced by ISIS into the Kurdistan Region of Iraq. Conflict and Health; 11:4. DOI 10.1186/s13031-017-0106-0
- UNDP Iraq Website. Promoting the Alignment of Development Plans with the Sustainable Development Goals. Posted on 29 October 2018. http://www.iq.undp.org/content/iraq/en/home/presscenter/pressreleases/2018/10/29/promoting-the-alignment-of-development-plans-with-the-sustainabl.html
- WHO. Refugees and Internally Displaced Persons in the Eastern Mediterranean Region: A Health Perspective. Cairo: WHO; 2015
- Ministry of Planning Kurdistan Regional Government. Kurdistan Region of Iraq 2020. A Vision for the Future
- Moramarco S, Basa FB, Alsilefanee HH, et al. 2019. Developing a Public Health Monitoring System in a War-torn Region: A Field Report from Iraqi Kurdistan. Disaster Medicine and Public Health Preparedness 5:1-3. doi: 10.1017/dmp.2019.116
- Emberti Gialloreti L, Basa FB, Moramarco S, Salih AO, Alsilefanee HH, Qadir SA, et al. 2020. Supporting Iraqi Kurdistan Health Authorities in Post-Conflict Recovery: The Development of a Health Monitoring System. Frontiers in Public Health; 8 (7)
- Emberti Gialloreti L, Moramarco S, Palombi L. Investing in Epidemiological Surveillance for Recovering Health Systems in War-Torn Countries. 2020. Perspectives in Public Health;140(1):25-26. doi: 10.1177/1757913919872514